As part of a series on Pulse, Dr Yassir Javaid, a GPwSI in cardiology and echocardiography, asks what these ECGs could signify. See bottom of the page for answers
Question 1
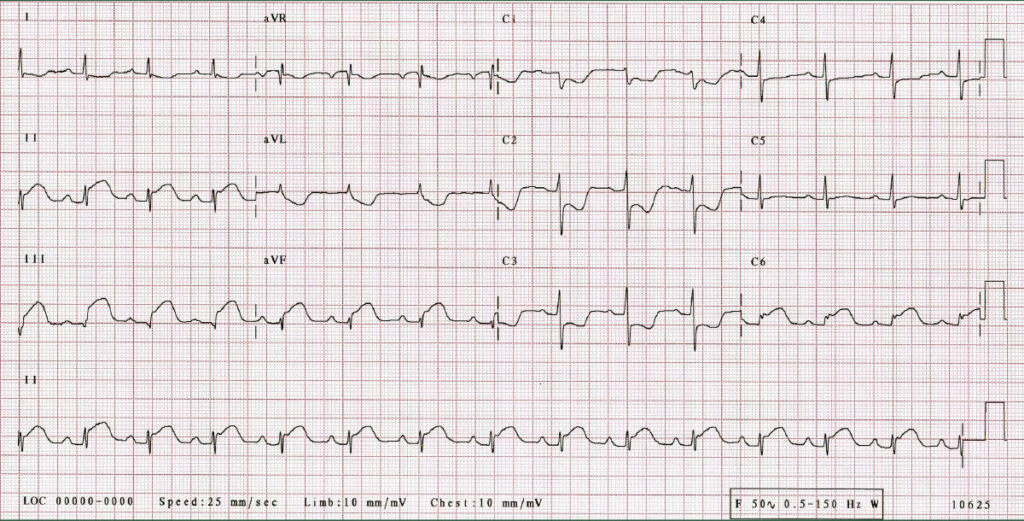
66 year old woman presents with chest tightness and nausea. She has a history of diabetes and is a smoker. The ECG is consistent with which ONE of the following diagnoses?
A Acute pericarditis
B Acute ST elevation inferior (and possibly posterior) MI
C Acute anterior ST depression MI with reciprocal inferior ST elevation
D Brugada pattern
E Benign early repolarization
Question 2
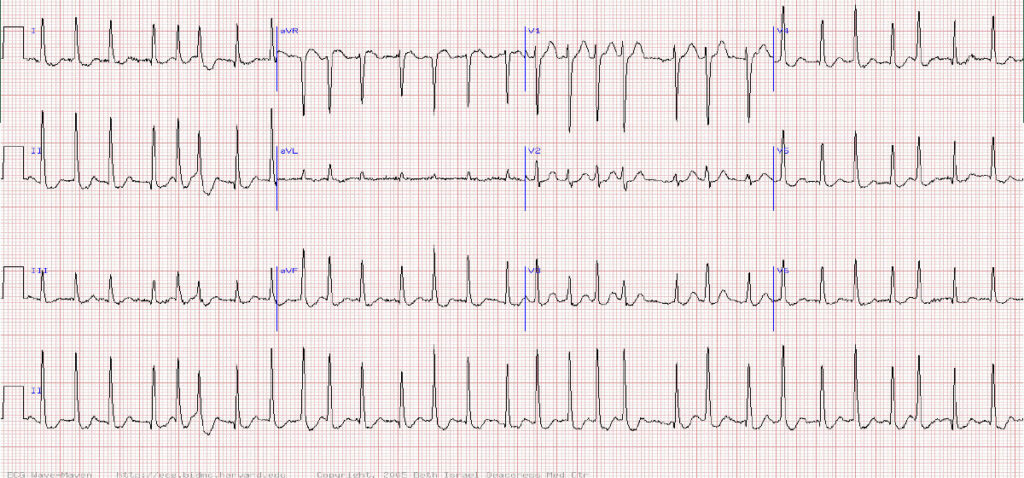
A middle-aged woman present with recent onset fast palpitations. This arrhythmia is most consistent with which endocrine disorder?
A Hyperthyroidism
B Hypothyroidism
C Hyperparathyroidism
D Addison’s disease
E Cushing’s disease
Question 3
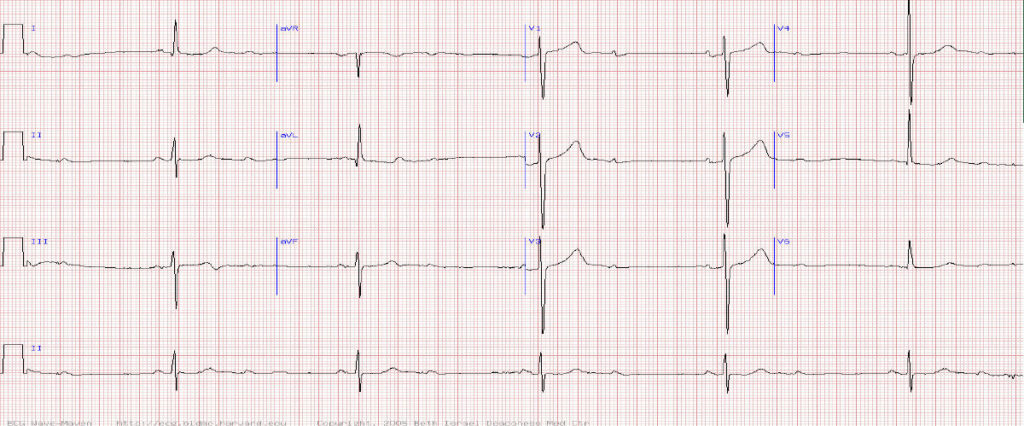
85-year-old male is worried about a slow heart rate but is without symptoms and is not on cardiac medications. What is the rhythm here?
A Atrial tachycardia with AV block
B Sinus bradycardia (marked) consistent with sick sinus syndrome
C Sinus rhythm with 2:1 AV block
D Sinus rhythm with complete (third degree) AV block
E Sinus rhythm with 3:2 AV Wenckebach
Answers
Question 1 Acute ST elevation inferior (and possibly posterior) MI
Explanation
Any history suggestive of possible acute coronary syndrome should warrant a 999 admission to hospital irrespective of ECG findings. However it would be reasonable to do an ECG at the surgery whilst waiting for an ambulance and have a defibrillator on standby.
The ECG reveals significant ST changes in the inferior leads – ie ST elevation in leads II, III, aVF
TIP Be aware of the regions of the heart within an ECG ie anterior = V1-V4, lateral = I, aVL, V5 & V6, inferior = II, III and aVF. If you find similar abnormalities within the leads of a region that is highly suspicious of ischaemic pathology.
Question 2 Hyperthyroidism
Explanation
The ECG clearly shows a tachyacardia, the absence of p waves and an irregular QRS rhythm confirming fast atrial fibrillation. The other clue is the variation in amplitude of the QRS complexes. The single wave seen between the QRS complexes must be a T wave as every QRS complex must be accompanied by a T wave – you cant have ventricular depolarization without ventricular repolarization.
Hyperthyroidism has a strong association with AF and can also contribute to the tachycardia. Correction of the hyperthyroidism can lead to resolution of the atrial fibrillation.
Question 3 Sinus rhythm with 2:1 AV block
Explanation
A slow heart rate can be physiological or pathological.
Physiological causes are always asymptomatic (eg young fit athletes) but pathological causes can be asymptomatic or symptomatic. Exclude betablockers or rate limiting calcium channel blockers (eg diltiazem) as a cause and consider whether there may be underlying hypothyroidism.
An ECG should be undertaken if a suspected pathological cause.
This ECG reveals regular P waves but only every other p wave is followed by a QRS complex indicating a high degree heart block – in this case 2nd degree type 2 with 2:1 AV conduction, This requires referral for assessment for a pacemaker
Pulse October survey
Take our July 2025 survey to potentially win £1.000 worth of tokens

Visit Pulse Reference for details on 140 symptoms, including easily searchable symptoms and categories, offering you a free platform to check symptoms and receive potential diagnoses during consultations.
Related Articles
READERS' COMMENTS [1]
Please note, only GPs are permitted to add comments to articles









Good article, but I would say it is medical student level.